A Phase II Trial of Asciminib, Dasatinib, Prednisone, and Blinatumomab for Participants with Newly Diagnosed Philadelphia Chromosome Positive (Ph+) Acute Lymphoblastic Leukemia
Anjali S. Advani, MD
&
Michaela Liedtke, MD
21CTP.LEUK01 Study Chairs
ACTIVATED: 5/15/2025
For sites that are members of the SWOG Cancer Research Network ONLY:
If your site is interested in applying to open this study, please complete the feasibility questionnaire. It collects essential information to help us assess each site’s suitability for the study.
21CTP.LEUK01 Study Synopsis
Schema
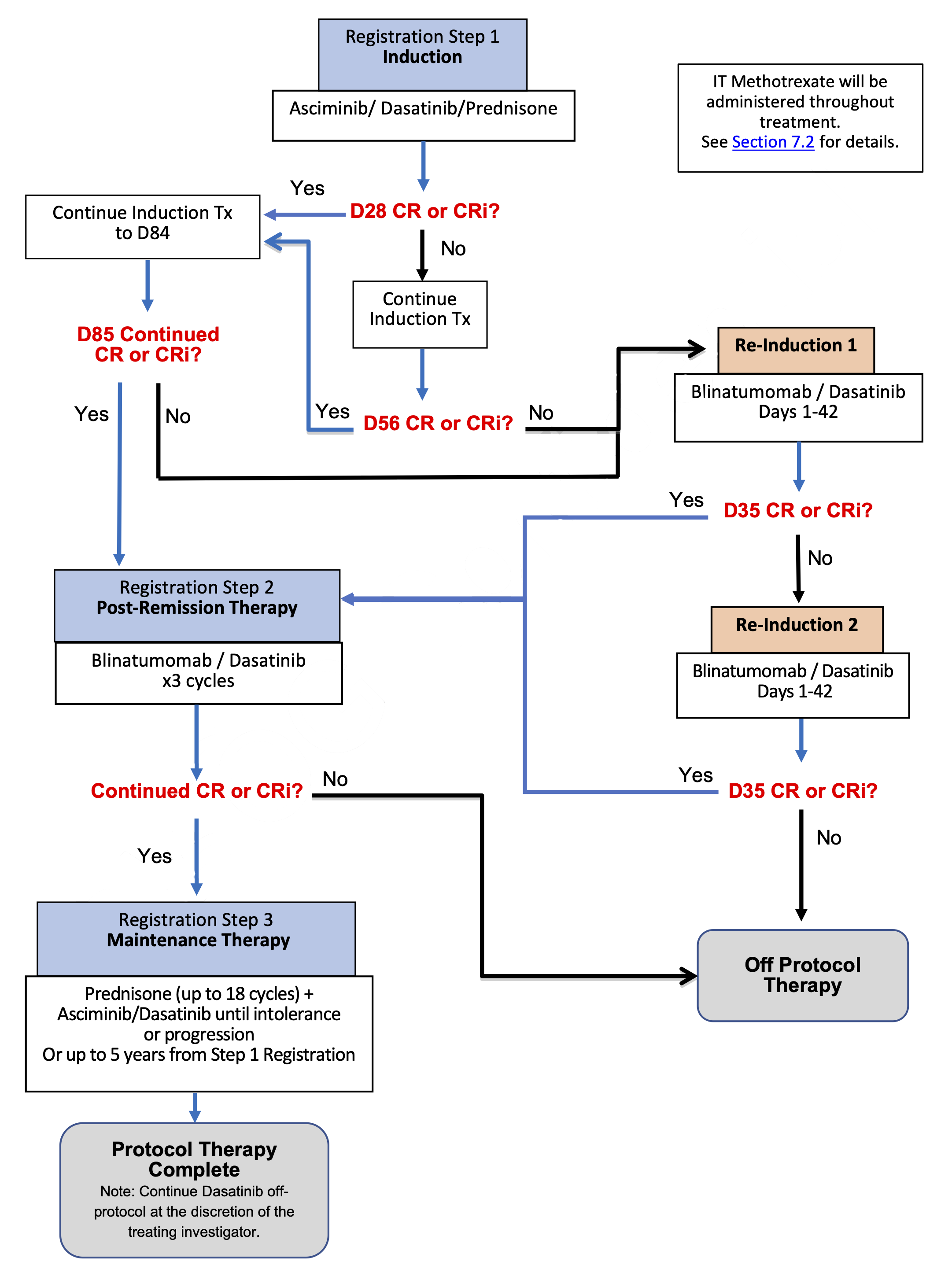
Objective
- To assess the rate of major molecular remission (MMR) by polymerase chain (PCR) for BCR-ABL at day 85 in newly diagnosed participants with Philadelphia-chromosome positive Ph+ acute lymphoblastic leukemia (ALL) treated with asciminib, dasatinib, and prednisone.
Key Eligibility
Inclusion Criteria
-
Newly diagnosed Ph+ ALL patients with presence of the BCR-ABL fusion detected by cytogenetics, FISH or PCR:
- age 60 or older OR
- younger than age 60 and not fit for intensive therapy
- Zubrod performance status 0-3
-
Calculated creatinine clearance ≥ 50mL/min using the Cockcroft-Gault Formula within 14 days prior to registration
- AST and ALT ≤ 3 x IULN within 14 days prior to registration
- Bilirubin ≤ 2 x IULN within 14 days prior to registration
- Ejection fraction ≥ 50% based on echocardiogram of MUGA
- QTcF < 500 ms (by Fridericia calculation) based on EKG performed within 28 days prior to registration
Exclusion Criteria
- No history or presence of clinically relevant CNS pathology such as epilepsy, seizure, paresis, aphasia, stroke, severe brain injuries, dementia, Parkinson’s disease, cerebellar disease, organic brain syndrome, psychosis, active ALL in the CNS confirmed by CSF analysis, or other significant CNS abnormalities.
- Patients must not have received any prior chemotherapy, investigational agents, radiation therapy, or other therapy for the treatment of ALL other than the following for a maximum of 7 days: FDA-approved TKI therapy, steroids, hydroxyurea, leukapheresis, and intrathecal chemotherapy.
- Systemic fungal, bacterial, viral, or other infection that is not controlled (defined as exhibiting ongoing signs/ symptoms related to the infection and without improvement despite appropriate antibiotics or other treatment).
- Patients must not have clinically significant autoimmune disease.
- Patients with known history of (HIV)-infection must be on effective anti-retroviral therapy at registration and have undetectable viral load test on the most recent test results obtained within 6 months prior to registration.
- Patients must not have a prior or concurrent malignancy whose natural history or treatment has the potential to interfere with the safety or efficacy assessment of the investigational regimen.
- Patients must discontinue proton pump inhibitors at the initiation of treatment.
- Patients must not have a history of or current acute pancreatitis, chronic pancreatitis, or any ongoing pancreatic disease.
-
Study Calendars
These study calendars are based on the January 22, 2025, protocol version. Always refer to the latest IRB-approved protocol.
Study Calendar 9.1 Registration Step 1 — Induction
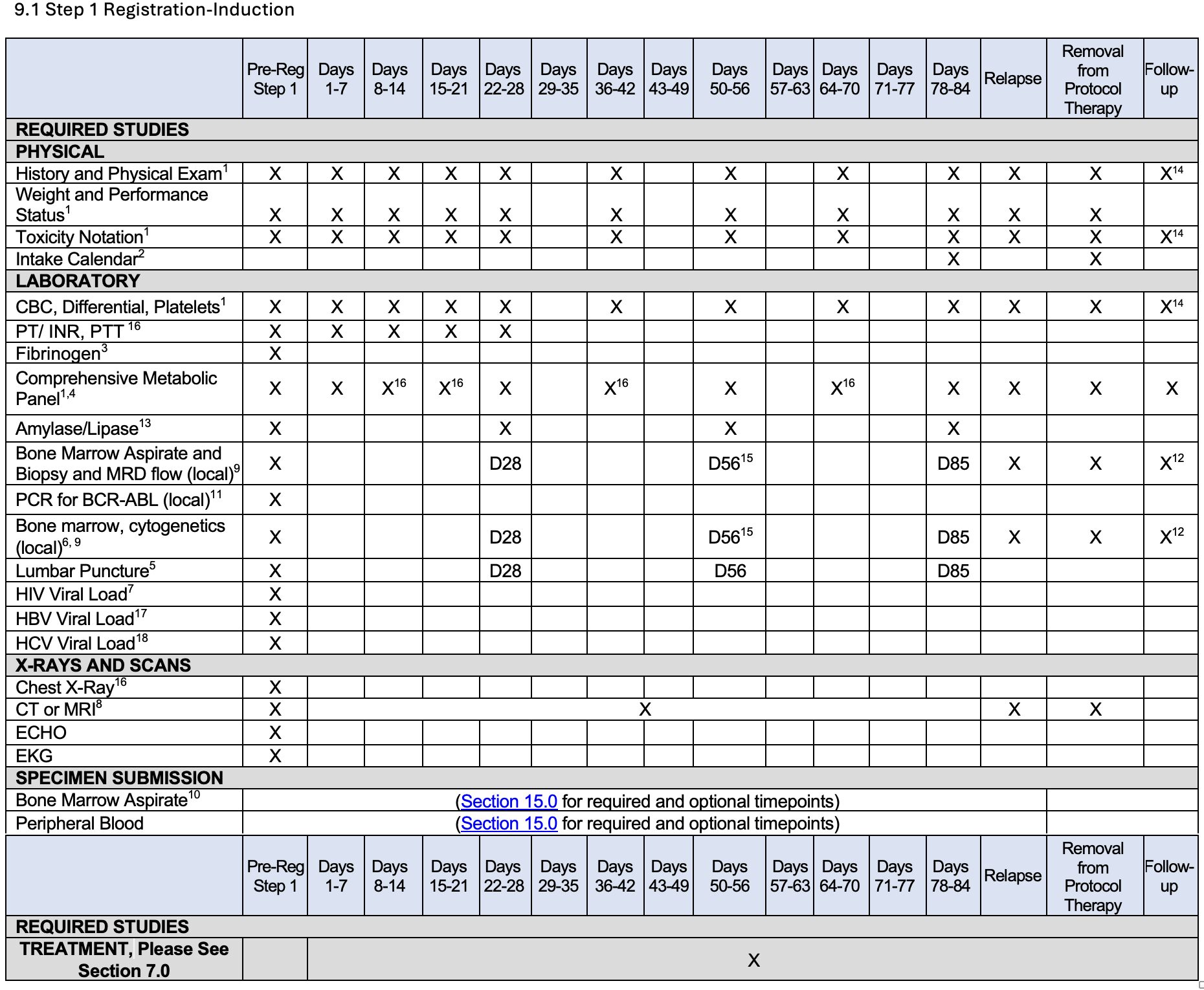
Footnotes for 9.1, Registration Step 1 – Induction
NOTE: Unless indicated otherwise in the protocol, scheduled procedures and assessments (treatment administration, toxicity assessment for continuous treatment, disease assessment, specimen collection and follow-up activities) must follow the established SWOG guidelines as outlined in https://www.swog.org/clinical-trials/protocol-workbench.
Note: Forms are found on the SWOG website (www.swog.org ). The schedule for submission of these forms is listed in Section 14.0.
- Performed pre-study, weekly Days 1-28 and every other week between Days 29-84 while on protocol treatment, and then every follow-up study visit post-treatment.
- CRA will review intake calendar at the end of each cycle (see Section 18.2).
- Performed pre-study, then as clinically indicated Days 1-28.
- Institutional standard metabolic panel is sufficient, provided it includes total bilirubin, AST and/or ALT, serum creatinine and alkaline phosphatase. Once off protocol treatment, every 3 months for the first year until LFTs are normal, and from years 2-5 from Step 1 Registration, as clinically indicated.
- LP with intrathecal (IT) chemotherapy prophylaxis approximately monthly for a total of 12 doses. CSF studies only need to be sent pre-registration to determine CNS status.
- Cytogenetics must be done within 28 days prior to registration, then subsequently at any time a bone marrow biopsy is performed for disease assessment (see Section 5.1b ).
- Required for participants with a known history of HIV (see Section 5.1c.)
- Only if there is evidence of extramedullary disease at diagnosis, CT scan or MRI of the chest, abdomen and pelvis will be performed pre-study, then every 3 months while on protocol treatment until CT/MRI is negative for extramedullary disease. CT/MRI is also required at relapse and at the time the participant is removed from protocol therapy for any reason.
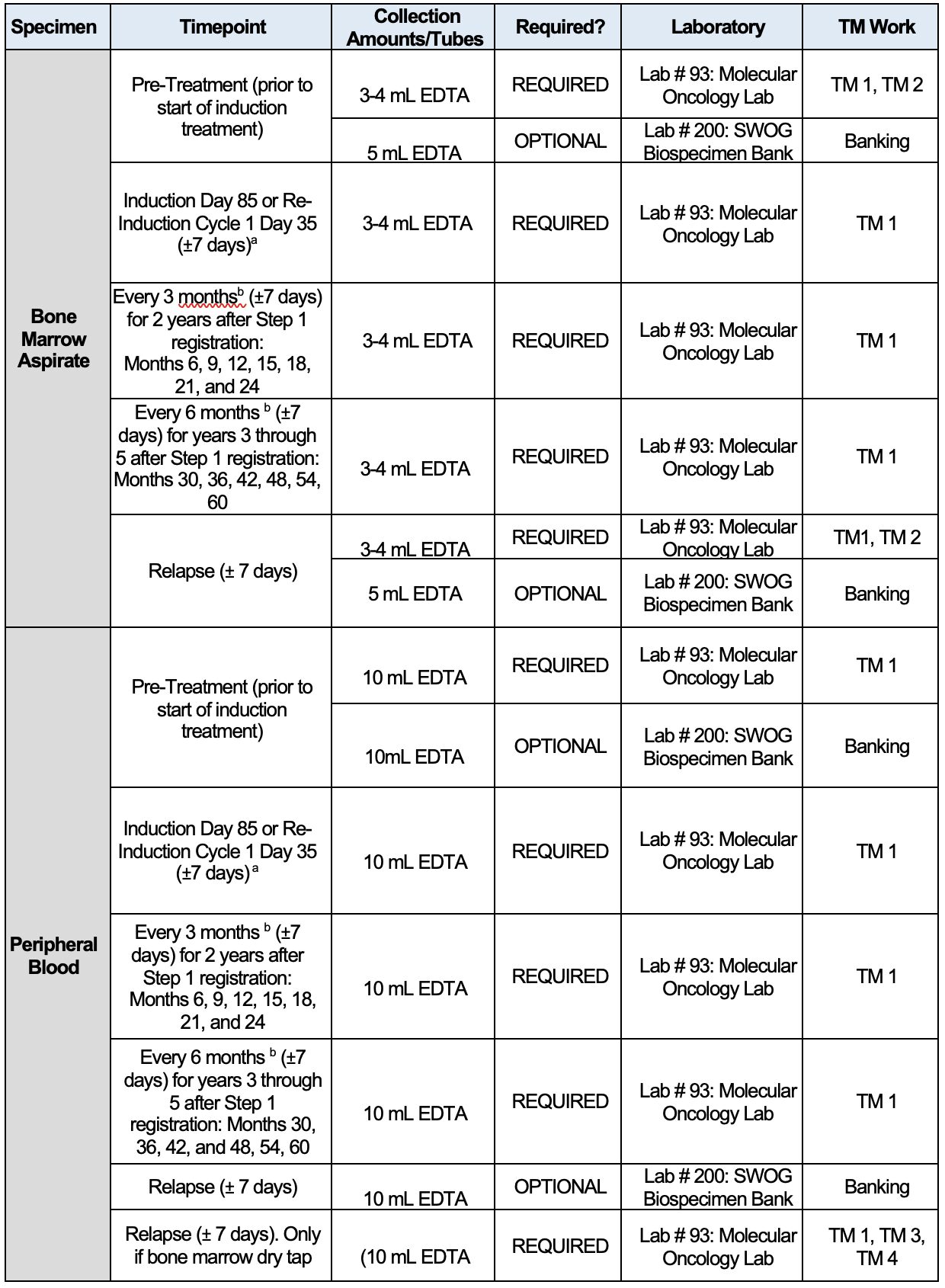
- Specimen collection to be performed +/-7 days of each timepoint.
- Mandatory bone marrow aspirate must be obtained every 3 months for 2 years, then every 6 months for years 3 through 5 after Step 1 Registration for TM studies (See Section 15.2).
- PCR for BCR-ABL (both p190 and p210 analyses) must be performed within 28 days prior to registration. Subsequent analyses for RT-PCR BCR-ABL will be performed centrally. See Section 15.2 for required specimen submissions.
- At discretion of treating physician.
- At Pre-Registration Step 1 then monthly while on induction therapy.
- Once off protocol treatment, participants must be followed every 3 months for the first two years, and then every 6 months until 5 years from Step 1 Registration.
- Day 56 assessment is only required if participant does not achieve CR/CRi at D28.
- If clinically indicated.
- Please see Section 5.1.c.11.
- Please see Section 5.1.c.13.
Study Calendar 9.2 Re-Induction
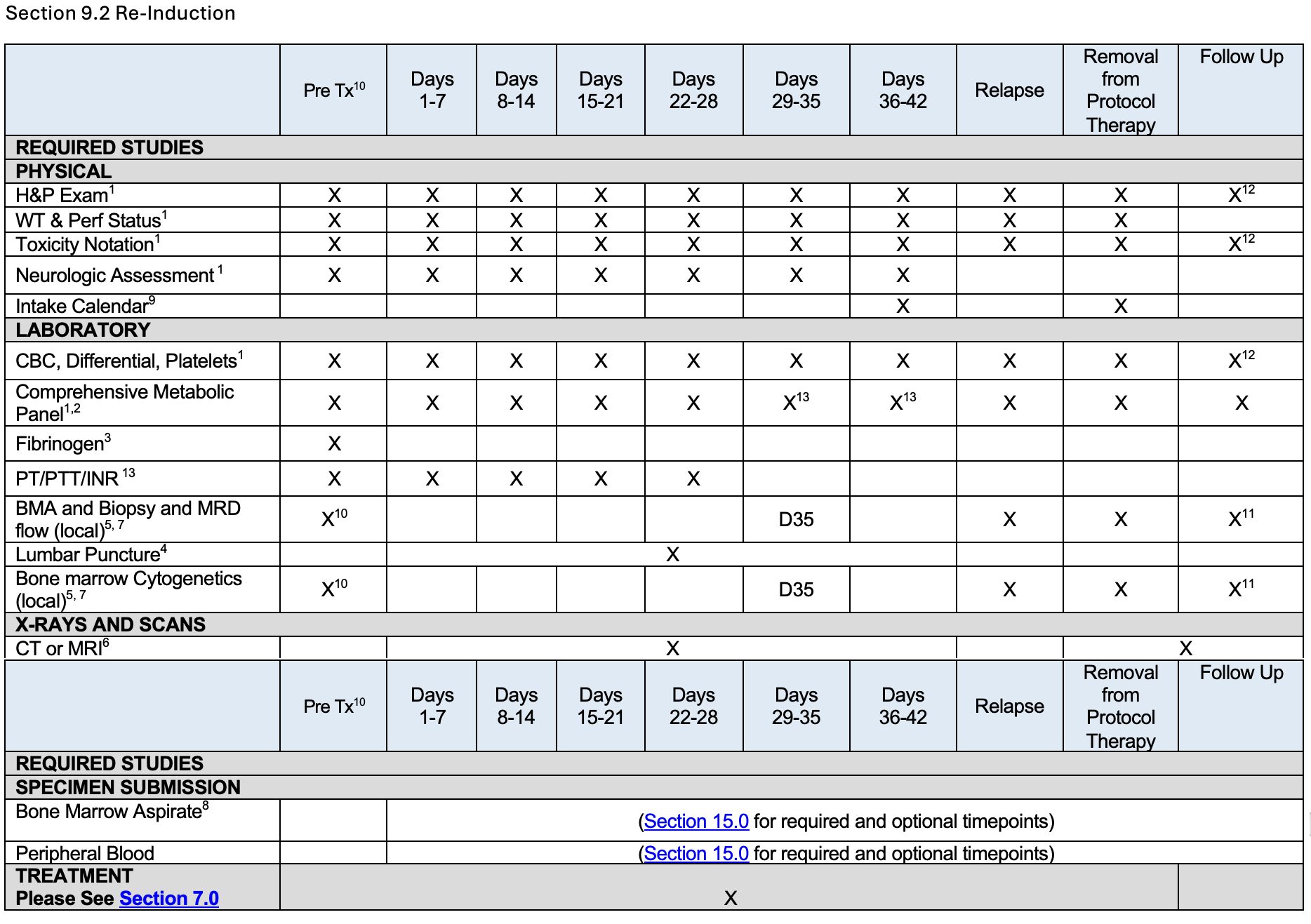
Footnotes for 9.2, Re-Induction
Note: Forms are found on the protocol abstract page of the SWOG website (www.swog.org ). The schedule for submission of these forms is listed in Section 14.0.
- Performed once weekly while on protocol treatment, and then every follow -up study visit post treatment.
- Institutional standard metabolic panel is sufficient, provided it includes total bilirubin, AST and/or ALT, serum creatinine and alkaline phosphatase. Once off protocol treatment, every 3 months for the first year until LFTs are normal, and from years 2-5 from Step 1 Registration, as clinically indicated.
- Performed pre-treatment, then as clinically indicated during Days 1-28.
- LP with IT chemotherapy prophylaxis approximately monthly for a total of 12 doses. Please see Section 7.2.d.
- Cytogenetics must be done at any time a bone marrow biopsy is performed for disease assessment (see Sections 5.1 ).
- Only if there is evidence of extramedullary disease at diagnosis, CT scan or MRI of the chest, abdomen and pelvis will be performed pre-study, then every 3 months while on protocol treatment until CT/MRI is negative for extramedullary disease. CT/MRI is also required at relapse and at the time the participant is removed from protocol therapy for any reason.
- Specimen collection to be performed +/-7 days of each timepoint.
- Mandatory bone marrow aspirate must be obtained every 3 months for 2 years, then every 6 months for years 3 through 5 after Step 1 Registration for TM studies (See Section 15.2).
- CRA will review intake calendar at the end of each cycle (see Section 18.2).
- Bone marrow biopsy and aspirate do not need to be repeated if performed within 2 weeks. All other assessments must be performed within 1 week.
- At discretion of treating physician.
- Once off protocol treatment, participants must be followed every 3 months for the first two years, and then every 6 months until 5 years from Step 1 Registration.
- If clinically indicated.
Study Calendar 9.3 Registration Step 2 Post-Remission
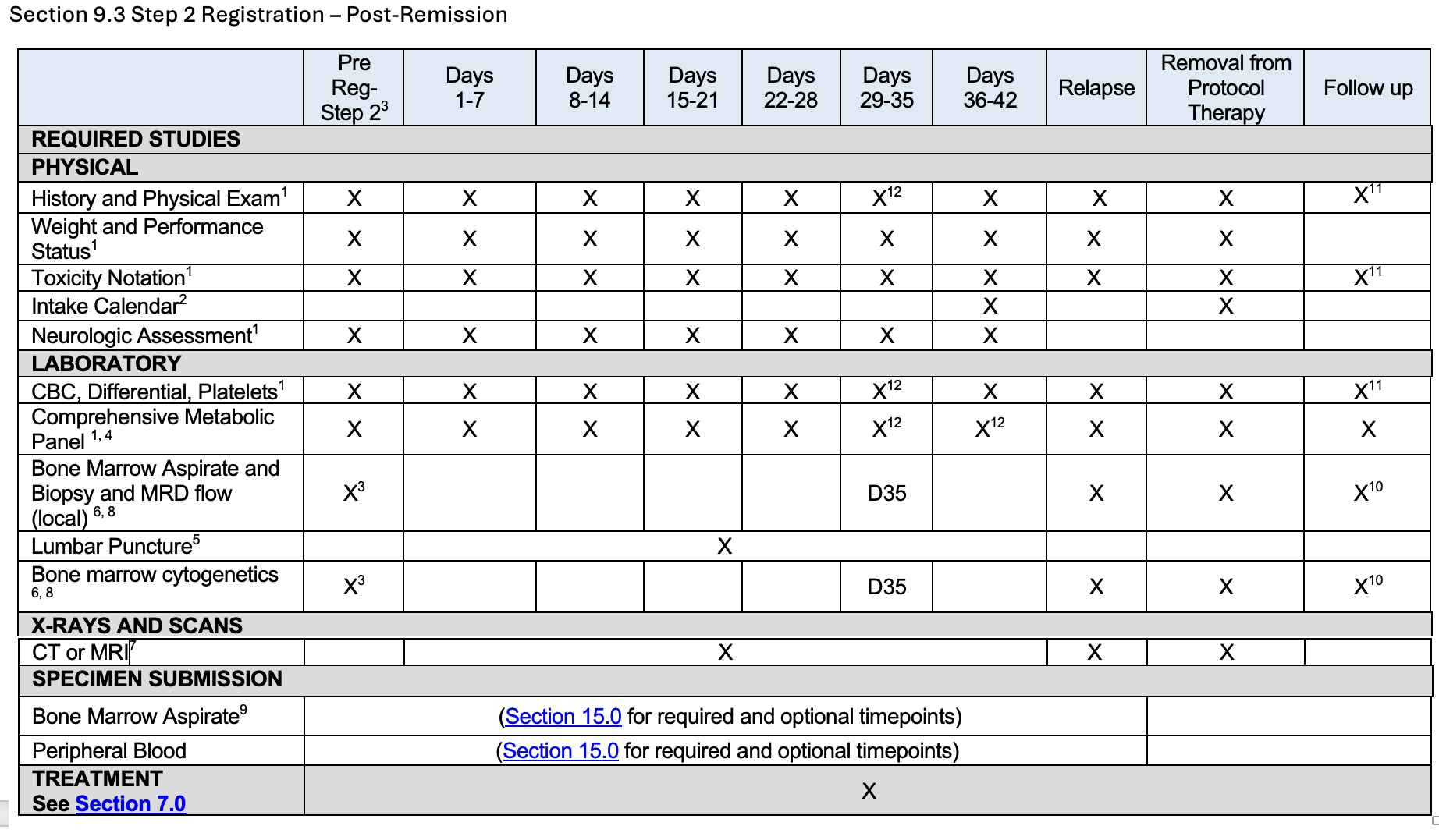
Footnotes for 9.3, Registration Step 2 Post-Remission
Note: Forms are found on the protocol abstract page of the SWOG website (www.swog.org ). The schedule for submission of these forms is listed in Section 14.0.
NOTE: Unless indicated otherwise in the protocol, scheduled procedures and assessments (treatment administration, toxicity assessment for continuous treatment, disease assessment, specimen collection and follow-up activities) must follow the established SWOG guidelines as outlined in https://www.swog.org/clinical-trials/protocol-workbench.
- Performed once weekly while on protocol treatment, and then every follow-up study visit post treatment.
- CRA will review Intake Calendar at the end of each cycle (see Section 18.2).
- Bone marrow biopsy and aspirate do not need to be repeated if performed within 4 weeks. All other assessments must be performed within 1 week.
- Institutional standard metabolic panel is sufficient, provided it includes total bilirubin, AST and/or ALT, serum creatinine and alkaline phosphatase. Once off protocol treatment, every 3 months for the first year until LFTs are normal, and from years 2-5 from Step 1 Registration, as clinically indicated.
- LP with IT prophylaxis approximately monthly for a total of 12 doses.
- Cytogenetics must be done at any time a bone marrow biopsy is performed for disease assessment (see Section 5.1 ).
- Only if there is evidence of extramedullary disease at diagnosis, CT scan or MRI of the chest, abdomen and pelvis will be performed pre-study, then every 3 months while on protocol treatment until CT/MRI is negative for extramedullary disease. CT/MRI is also required at relapse and at the time the participant is removed from protocol therapy for any reason.
- Specimen collection to be performed +/-7 days of each timepoint.
- Mandatory bone marrow aspirate must be obtained every 3 months for 2 years, then every 6 months for years 3 through 5 after Step 1 Registration.
- At discretion of treating physician.
- Once off protocol treatment, participants must be followed every 3 months for the first two years, and then every 6 months until 5 years from Step 1 Registration.
- If clinically indicated.
Study Calendar 9.4 Registration Step 3 Maintenance
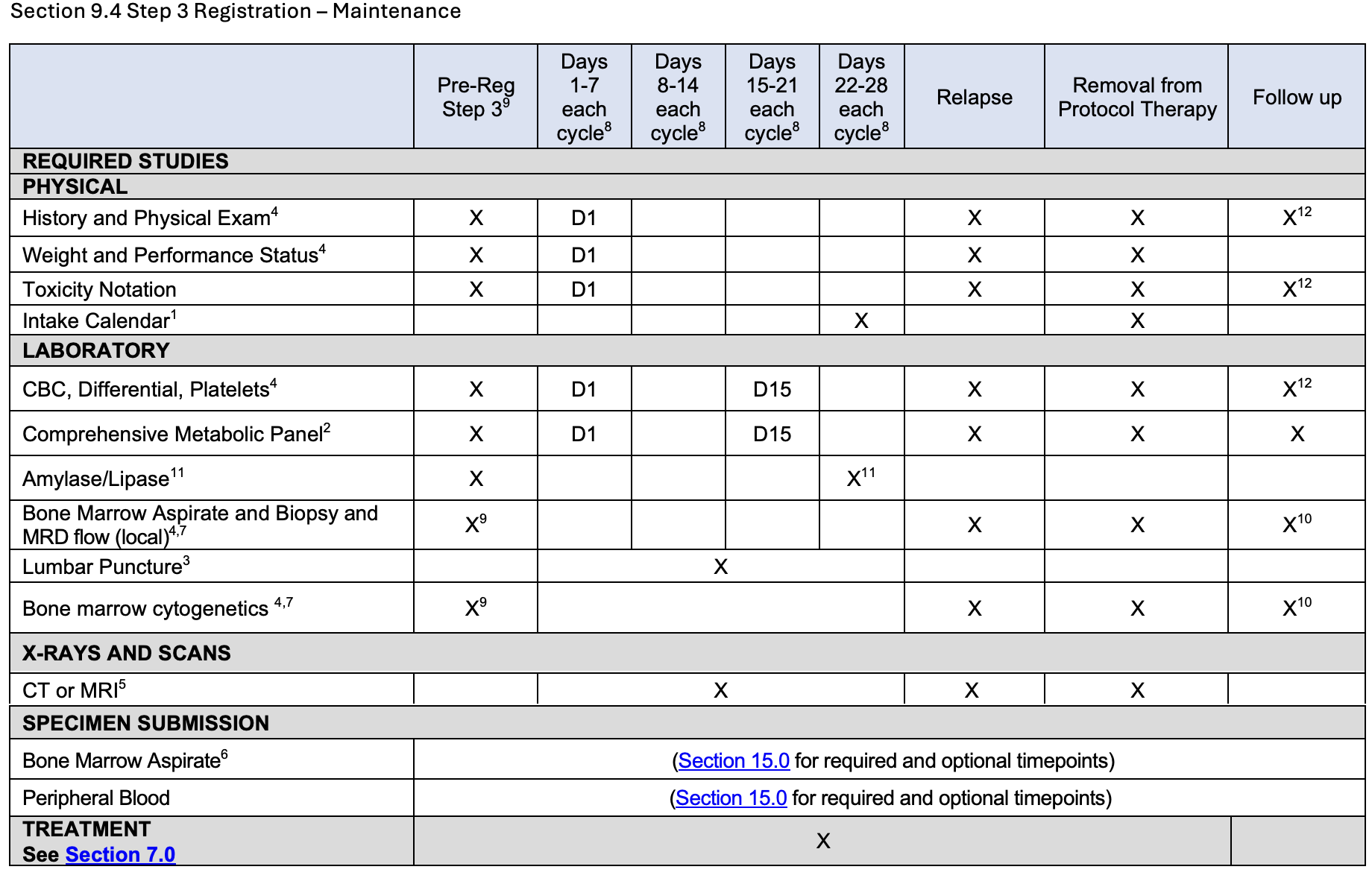
Footnotes for 9.4, Registration Step 3 – Maintenance
Note: Forms are found on the protocol abstract page of the SWOG website (www.swog.org ). The schedule for submission of these forms is listed in Section 14.0.
NOTE: Unless indicated otherwise in the protocol, scheduled procedures and assessments (treatment administration, toxicity assessment for continuous treatment, disease assessment, specimen collection and follow-up activities) must follow the established SWOG guidelines as outlined in https://www.swog.org/clinical-trials/protocol-workbench.
- CRA will review Intake Calendar at the end of each cycle (see Section 18.2)
- Institutional standard metabolic panel is sufficient, provided it includes total bilirubin, AST and/or ALT, serum creatinine and alkaline phosphatase. Once off protocol treatment, every 3 months for the first year until LFTs are normal, and from years 2-5 from Step 1 Registration, as clinically indicated.
-
LP with IT prophylaxis approximately monthly for a total of 12 doses.
-
Cytogenetics must be done at any time a bone marrow biopsy is performed for disease assessment (see Section 5.1b ).
-
Only if there is evidence of extramedullary disease at diagnosis, CT scan or MRI of the chest, abdomen and pelvis will be performed pre-study, then every 3 months while on protocol treatment until CT/MRI is negative for extramedullary disease. CT/MRI is also required at relapse and at the time the participant is removed from protocol therapy for any reason.
-
Mandatory bone marrow aspirate must be obtained every 3 months for 2 years, then every 6 months for years 3 through 5 after Step 1 Registration.
-
Specimen collection to be performed +/-7 days of each timepoint.
-
Additional Cycles up to 5 years from Step 1 Registration (except Prednisone, which is limited to 18 cycles).
-
Bone marrow biopsy and aspirate do not need to be repeated if performed within 4 weeks. All other assessments must be performed within 2 weeks.
-
At discretion of treating physician.
-
At Pre-Registration Step 3 then monthly while on maintenance therapy.
-
Once off protocol treatment, participants must be followed every 3 months for the first two years, and then every 6 until 5 years from Step 1 Registration.
Specimen Collection
Funding Memo
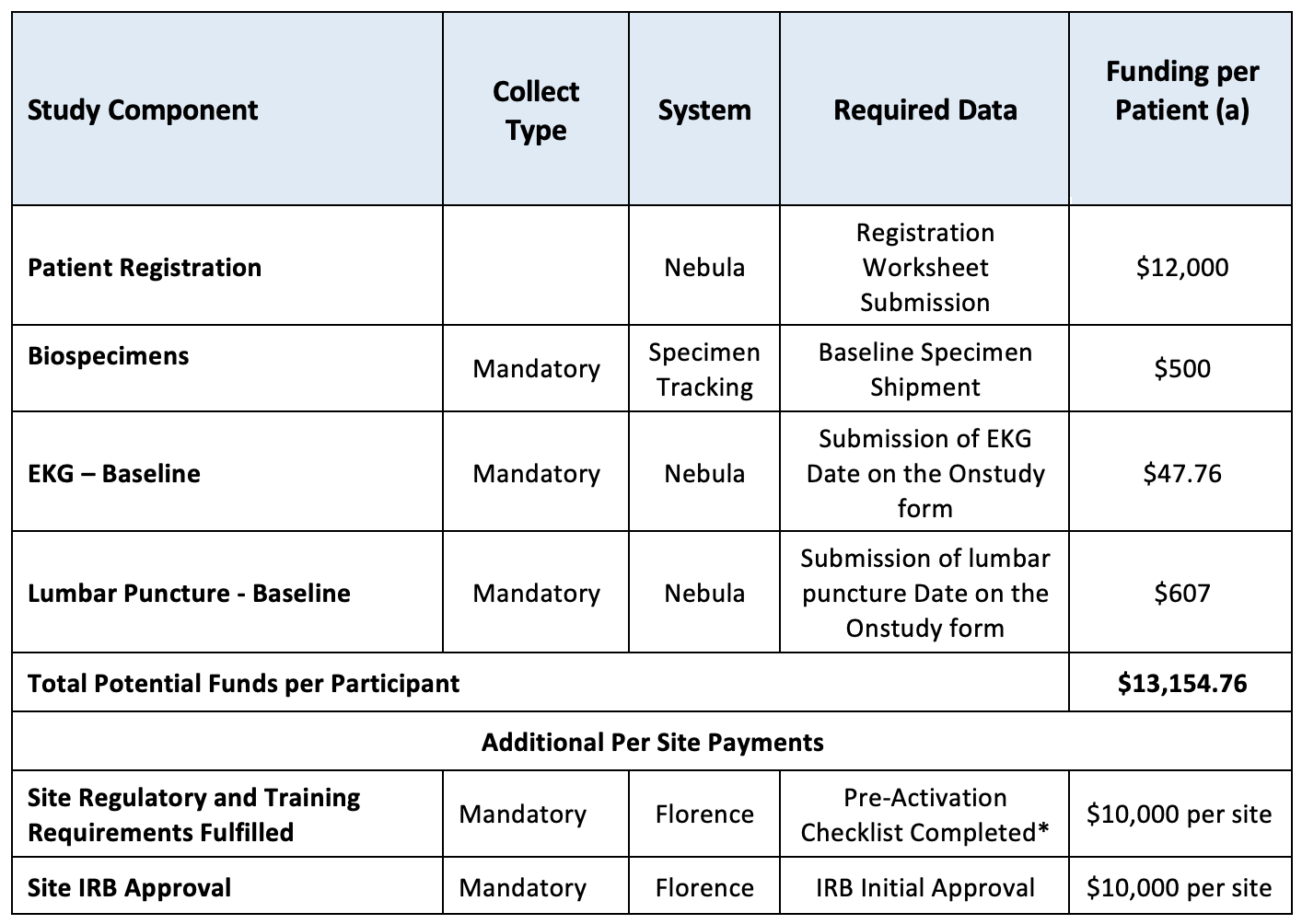
* Pre-Activation Checklist-
- Form FDA 1572
- DTL (Delegation of Tasks Log)
- CVs (curriculum vitae)
- FDFs (Financial Disclosure Forms)
- Medical Licenses
- GCP Training Certs.
- Florence Training Certs.
- Site Signature Page
Study Contact Information
Funding Questions:
[email protected]
Protocol Questions Contact:
[email protected]